You wake up, swing your legs over the side of the bed, take your first step — and something in your heel fires like a hot nail straight into the arch. A few minutes later it eases off. By mile two of your run it’s almost gone. Then you finish, cool down, sit at your desk for an hour — and it’s back.
That’s not “tight fascia from yesterday’s workout.” That’s plantar fasciitis — and it sidelines more runners than almost any other lower-limb injury. Research published in PMC puts the prevalence among runners at up to 17.4% of the entire running population. Over one million doctor visits a year in the United States alone.
The good news: the vast majority of cases resolve without surgery, injections, or stopping running entirely. The bad news: most runners drag it into a chronic state because they treat it the way runners treat everything — push through it and hope it goes away. It doesn’t work like that.
This article covers everything: what actually happens inside your foot, why runners are particularly vulnerable, and — most importantly — a concrete, evidence-based recovery plan you can start today.
- What Is Plantar Fasciitis?
- Plantar Fasciitis Symptoms: How to Recognize It
- Causes of Plantar Fasciitis in Runners
- Plantar Fasciitis Exercises and Stretching
- Tissue-specific plantar fascia stretch — the primary intervention
- Calf and Achilles complex stretching
- Intrinsic foot muscle strengthening
- Eccentric heel drops
- How to Treat Plantar Fasciitis: Evidence-Based Options
- Phase 1: Initial therapies (weeks 1–6)
- Phase 2: When initial treatment isn’t enough (6–8 weeks in)
- Phase 3: Persistent cases (6–12+ months)
- How to Prevent Plantar Fasciitis When Running
- The Bottom Line
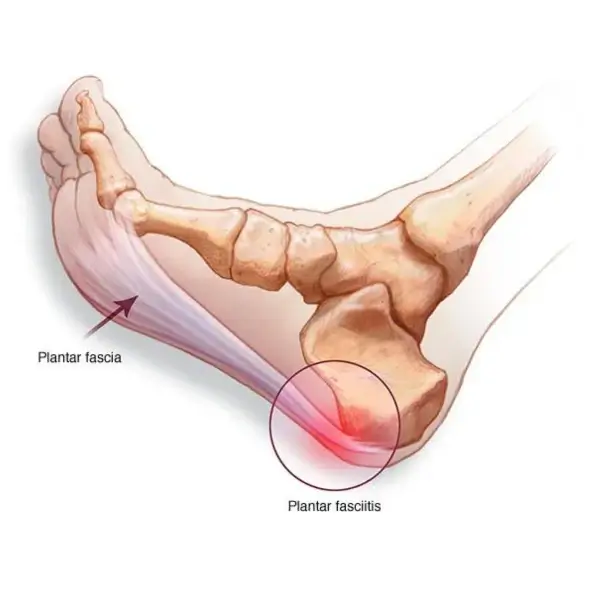
What Is Plantar Fasciitis?
The plantar fascia is a thick band of connective tissue running from the calcaneus — your heel bone — to the base of your toes. It does two jobs: support the longitudinal arch of the foot and act as a spring, storing and releasing energy with every step. Under normal load and with adequate recovery time, it handles this well. The problem starts when the cumulative stress exceeds its capacity to repair itself.
Here’s a nuance that most patient-facing articles get wrong: the word “fasciitis” implies inflammation. But histological studies consistently show that in chronic cases, there’s little to no active inflammation — what you actually have is degenerative tissue, micro-tears, and disorganized collagen. It’s closer mechanically to Achilles tendinopathy than to an acute inflammatory injury. This matters for treatment: anti-inflammatory strategies — ice, ibuprofen — are relevant in the early acute phase. Once you’re dealing with a chronic presentation, the treatment logic has to shift entirely toward tissue remodeling and load management.
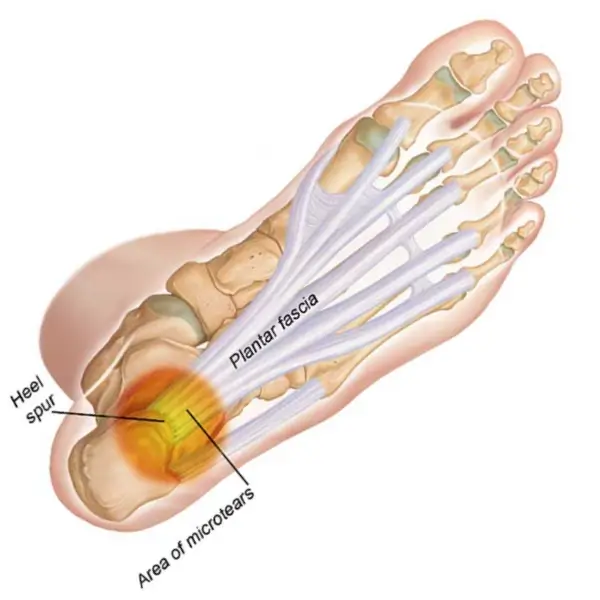
The mechanism is straightforward: repetitive stress → micro-tears at the fascial insertion on the heel bone → attempted repair → thickening of the fascia → pain during loading and especially during the first steps after rest, when the fascia is yanked taut from a shortened, contracted position.
How is it different from other heel pain? This is critical to establish before you start any treatment.
Tarsal tunnel syndrome produces burning and numbness along the inner ankle and sole — a nerve pain quality, not a mechanical one. A calcaneal stress fracture gives diffuse heel pain that worsens with all weight-bearing and doesn’t ease during activity — it needs an MRI to rule out. A heel spur is a radiological finding, not a diagnosis; 15–25% of asymptomatic people have one on X-ray. Achilles tendinopathy sits higher, at the insertion point of the tendon, not in the plantar surface.
If you’re unsure, get an ultrasound. It’s fast, inexpensive, and definitively shows fascial thickening and any partial tears.
Plantar Fasciitis Symptoms: How to Recognize It
The clinical picture is characteristic enough that an experienced sports medicine physician or running coach can form a working diagnosis from the description alone.
Pain with the first steps in the morning is the hallmark sign. Overnight, the fascia shortens in a plantarflexed position — especially if you sleep with your feet pointed. Inflammatory byproducts accumulate around the calcaneal insertion. The first step applies sudden tensile load to already irritated tissue. This is also why the standard advice is to stretch the fascia before you even get out of bed.
Pain after prolonged sitting or standing follows the same logic. You’ve been at your desk for an hour, fascia has shortened again, and standing applies that same abrupt load.
Pain that eases during a run but returns afterward is typical in early-to-moderate stages. The tissue warms up, local blood flow increases, pain threshold rises. But the underlying damage is still accumulating — the absence of pain during the run is not a signal that you’re recovering. It’s a signal that you’re in a window where continued loading feels tolerable while the pathology progresses.
Localization: sharp, point-specific pain on the medial (inner) aspect of the heel. Press your thumb into the front-inner part of the heel — if that’s exactly where it hurts, the picture is fairly clear.
When to see a doctor without delay:
- No improvement after 4–6 weeks of consistent self-treatment
- Swelling, redness, or local warmth around the heel
- Pain that doesn’t settle with rest or wakes you at night
- You have a race in 8–10 weeks and need to know what you’re actually dealing with
The last point isn’t trivial. If you’re mid-training-cycle, an ultrasound gives you real information — fascial thickness, integrity, presence of partial tears — that changes the management decision significantly.

Causes of Plantar Fasciitis in Runners
Why runners specifically? Because at running pace, the plantar fascia absorbs 1.5 to 3 times body weight with every foot strike. Multiply that across 15,000–20,000 steps in an hour-long run and it becomes obvious why the tissue can’t always keep up with the demand.
But mileage is just one variable. Here’s what actually breaks the fascia.
Foot biomechanics. Excessive pronation — the foot rolling inward on landing — increases tensile strain along the medial fascial border. High-arched feet (pes cavus) have reduced shock absorption, concentrating impact at the heel. Both mechanics elevate risk, through different mechanisms.
Tight calf complex and limited ankle dorsiflexion. This is the most underappreciated risk factor in runners. When ankle dorsiflexion is restricted — you can’t get adequate range of motion with the knee straight or bent — the foot compensates by pronating excessively, which transfers more load to the medial fascia. Runners with chronically tight gastrocnemius and soleus muscles are consistently overrepresented in plantar fasciitis populations. Check yours: standing 10–12 cm from a wall, can you touch your knee to the wall without lifting your heel? If not, you have a dorsiflexion deficit that needs to be addressed.
Weak intrinsic foot muscles. The small muscles that actively control the arch — the ones most runners never deliberately train — are often atrophied, particularly in runners who’ve always worn high-support shoes. When they’re not doing their job, the plantar fascia takes the structural load that muscles should be managing. A clinical trial (NCT05455645) looking specifically at long-distance runners found a direct correlation between intrinsic foot muscle atrophy and chronic plantar fasciitis.
Training errors. The 10% rule exists for a reason: increasing weekly mileage by more than 10% week-over-week is a classic plantar fasciitis trigger. So is a rapid transition to minimalist footwear without a graduated adaptation period, heavy track or road sessions without variation in surface, and insufficient recovery between hard training days.
Systemic factors. BMI is a well-documented risk factor — confirmed across multiple systematic reviews (PMC8705263). Every additional kilogram increases the per-step load on the foot. Age 40–60 sees slower tissue remodeling. Occupations requiring prolonged standing on hard floors add a chronic low-grade baseline stress that stacks with training load.
Plantar Fasciitis Exercises and Stretching
This is the core of the article — because targeted exercise and stretching is what produces durable recovery. Not injections. Not shockwave therapy alone. Not pain medication. Those are adjuncts. The mechanical work is the treatment.
Tissue-specific plantar fascia stretch — the primary intervention
A landmark randomized controlled trial published in the Journal of Bone and Joint Surgery (PubMed 12851352, n=101 patients with chronic plantar fasciitis) compared a plantar fascia–specific stretching protocol against the standard Achilles tendon stretch. After eight weeks, the fascia-specific group showed statistically significant improvements across all functional outcome measures. The difference was clinically meaningful, not marginal.
Technique: Sit down and cross your affected foot over the opposite knee. Grip your toes and pull them back toward your shin until you feel a clear stretch along the arch of the foot. Hold for 10 seconds. Do 10 repetitions. Repeat three times a day — the first set before you take your first step in the morning, while you’re still sitting on the edge of the bed.
This requires no equipment, costs nothing, and takes three minutes. It is also the intervention most runners skip because it doesn’t feel like “enough.” It is enough — consistently applied.
Calf and Achilles complex stretching
Two variations, both essential:
Straight-leg calf stretch (gastrocnemius): Stand facing a wall, step one foot back with the knee straight and heel flat on the floor. Lean your hips forward until you feel the stretch in the upper calf. Hold 30 seconds, 3 sets per side.
Bent-knee calf stretch (soleus): Same setup, but with the back knee slightly bent. The stretch drops lower and deeper — into the soleus, which most runners never adequately target. Hold 30 seconds, 3 sets per side.
If your dorsiflexion test failed, treat this block as your highest priority. The exercises in this section are correcting the upstream mechanical cause of why the fascia is being overloaded in the first place.
Intrinsic foot muscle strengthening
Based on the clinical evidence from runners with chronic plantar fasciitis, progressive intrinsic muscle strengthening over 8 weeks significantly improves both symptom levels and foot function.
Short foot exercise: Without curling your toes, try to shorten your foot by drawing the ball of the foot toward the heel — the arch actively rises. This is difficult at first and the movement is small. 3 sets of 15, standing progressing to single-leg when you master it.
Towel curls: Lay a small towel flat on the floor and scrunch it toward you using only your toes. 3 sets of 10.
Marble or object pick-up: Pick up small objects from the floor with your toes and drop them into a cup. Good for motor control and smaller intrinsic muscles.
Eccentric heel drops
Stand on the edge of a step on the balls of both feet. Rise onto both toes. Shift weight to the affected foot only and slowly lower the heel below the step level — count 4 seconds down. Return to start using both feet. 3 sets of 15.
This protocol originated in Achilles tendinopathy rehabilitation but applies directly to plantar fasciitis: eccentric loading drives collagen remodeling in chronically degenerated fascial tissue. Start this only once acute pain has settled — meaning it’s not painful to walk normally.
How to Treat Plantar Fasciitis: Evidence-Based Options
A comprehensive review published in 2025 (PMC12294660) analyzed 30 separate treatment modalities across four management phases, drawing from PubMed and Cochrane data from 2020–2025. The conclusion: over 90% of plantar fasciitis cases resolve conservatively within 6–18 months. “Conservatively” does not mean passively. It means systematic, structured management.
Phase 1: Initial therapies (weeks 1–6)
Relative rest — not complete cessation of activity, but reducing load to a level at which you have no pain during and no pain the morning after training. Pool running, cycling, and elliptical training maintain cardiovascular fitness without axial loading on the fascia.
Ice — 15–20 minutes post-training. Effective symptom management in the early, more acute phase.
Orthotics — semi-rigid prefabricated insoles with arch support reduce medial fascial strain in pronators. Custom orthotics are indicated when there’s a meaningful biomechanical abnormality that off-the-shelf options don’t address.
Night splints — hold the foot in neutral or slight dorsiflexion during sleep, preventing overnight fascial shortening. Uncomfortable for the first few nights; effective at eliminating the morning first-step pain that otherwise keeps reinjuring the insertion every day.
NSAIDs — ibuprofen or naproxen provide short-term symptomatic relief in the early phase. They don’t address the underlying pathology and shouldn’t be used as a long-term strategy.
Phase 2: When initial treatment isn’t enough (6–8 weeks in)
Extracorporeal shockwave therapy (ESWT). A 2024 study specifically with runners (PMC11123367) demonstrated a dose-dependent effect of radial ESWT: progressively escalating intensity across treatment sessions produced significantly better outcomes in fascial biomechanical parameters than a fixed-dose protocol. Shockwave works by stimulating neovascularization and triggering collagen remodeling in chronically degenerated tissue that no longer responds to conservative measures alone. Typically 3–5 sessions, one week apart.
Corticosteroid injections. The numbers here are important. A prospective RCT (PubMed 40786809, n=100) showed injections were superior at weeks 2 and 6 — faster initial pain relief and functional improvement. But at weeks 12 and 16, the stretching group showed significantly better outcomes. There’s also a real risk of fascial rupture with repeated injections. The clinical implication: injections are a short-term pain management tool that can help you engage in rehabilitation — they are not a standalone treatment, and certainly not a substitute for the mechanical work.
Phase 3: Persistent cases (6–12+ months)
PRP (platelet-rich plasma) injections — inject concentrated growth factors from the patient’s own blood directly into the degenerated fascia to stimulate tissue repair. Evidence is moderate but consistently positive for cases that haven’t responded to first-line treatment.
Dry needling — addresses the myofascial component: trigger points in the calf, soleus, and intrinsic foot muscles that perpetuate loading patterns driving the fascial injury.
Endoscopic plantar fascia release — surgical option reserved exclusively for refractory plantar fasciitis not responding to 12+ months of comprehensive conservative treatment. This is a last resort, not a shortcut.
How to Prevent Plantar Fasciitis When Running
If you’re currently in recovery, this section is about making sure you don’t come back here. If you haven’t been injured yet, it’s about making sure you don’t.
Manage your mileage increase strictly. No more than 10% per week. This applies to experienced runners too — in fact, it applies especially to experienced runners who think they can tolerate more because they’ve been at it for years. Plantar fasciitis is frequently earned in marathon training build-ups where the weekly mileage spikes.
Vary your surfaces. Concrete and asphalt are the hardest surfaces you can run on. Trail, treadmill, grass, and track reduce impact load significantly. If your running is predominantly urban, compensate with footwear that provides adequate cushioning for the surface you’re on.
Replace your shoes on schedule. The midsole foam that provides cushioning degrades well before the outsole shows obvious wear. General guidance: 600–800 km. A practical signal: if late in a long run your heel starts to feel harder contact with the ground than it used to — your shoes are past their useful life for you.
Stretch before your first step every morning. This is the lowest-effort, highest-return habit in plantar fasciitis prevention. Sitting on the edge of the bed, pull your toes back toward your shin, hold 10 seconds, do it three times. Thirty seconds. It directly addresses the mechanism that creates micro-tears at the fascial insertion — the abrupt tensile load of a first step on a contracted, unwarmed fascia.
Train your weak links. If you have limited dorsiflexion, a tight calf complex, a weak arch, or excessive pronation — those are the things that need deliberate work in your training, not just mileage and speed sessions. Most runners spend zero time on this and wonder why the same injury keeps recurring.
Return to running correctly after injury. The criterion is simple: no pain while walking → start run/walk intervals. No pain during and no pain the following morning → progress. Pain returns → step back. No races, no tempo work, no long runs until you’ve passed through this protocol without symptoms. Every week you respect this process is a week that brings you back to full training. Every week you skip it is a week that extends your timeline.
The Bottom Line
Plantar fasciitis is not a sentence and it’s not something you just manage indefinitely. But it’s also not a self-resolving injury you can train through at full intensity while waiting for it to disappear.
Four things produce durable recovery: consistent plantar fascia–specific stretching (especially before your first step each morning), calf complex stretching to restore dorsiflexion, progressive intrinsic foot muscle strengthening, and reducing training load to a level that allows tissue adaptation to keep pace with stress.
A runner who addresses it early — in the first two to four weeks — typically returns to full training in four to six weeks. A runner who pushes through for three months and arrives with a chronic presentation is looking at six to eighteen months. The math strongly favors acting early.
If you’re planning your return to training and want to build your mileage back up without re-loading the fascia too quickly, use the training load calculator at calcrun.net to structure your progression.
Medical disclaimer. This article is for informational and educational purposes only and does not constitute medical advice. If you are experiencing symptoms of plantar fasciitis, consult a qualified physician, sports medicine specialist, or physiotherapist for an accurate diagnosis and individualized treatment plan.
Medical sources and references:
- NIH StatPearls — Plantar Fasciitis (continuously updated clinical review)
- PMC12294660 — Comprehensive Evidence-Based Treatment Framework 2025
- PMC8705263 — Systematic Review of systematic reviews: epidemiology, diagnosis, treatment
- PubMed 12851352 — Tissue-specific plantar fascia stretch RCT (JBJS)
- PMC10467524 — Physiotherapeutic interventions systematic review 2023
- PMC11123367 — Dose-escalation rESWT in runners 2024
- PubMed 40786809 — Stretching vs corticosteroid injections RCT
- PMC8956500 — Gastrocnemius-Soleus stretching program RCT